Man Bad
“Rupert Murdoch is ‘not a fit person’ to exercise stewardship of a major international company, a committee of MPs has concluded, in a report highly critical of the mogul and his son James’s role in the News of the World phone-hacking affair.”
— Get out!
Happy May Day and Let's Be Careful Out There

After last night’s disgusting “police visits” to activists’ homes (and the FBI went door-knocking too!) you can pretty much be sure today’s May Day demonstrations are going to be a doozy of police overreaction and unfortunate choices. Above, a screenshot from lower Manhattan. (JK, that’s the new Dark Knight trailer from last night. But don’t watch it, because you’ll be buying something with your eyes on Buy Nothing Day if you do!)
Around New York City, expect Union Square to be full of bicyclists right about now, busy all day and then filled with Das Racist circa 5 p.m.; Williamsburg Bridge will be closed late morning; and then the greater Wall Street area will be a mess after dark. (For another city near you, to join in or avoid, as you wish, check here.) This is a good list of what to think about before you attend any sort of demonstration, even the permitted ones. Some prefer the tactic of not giving identification to police, but if you are in New York City today and you run even the slightest risk of being arrested, I urge you to let friends know where you are and to carry ID with you. It’ll make your processing far, far easier.
Even if you stay home, you can expect to see some protest.
Welcome to #MayDay. Expect Us. #Anonymous #OWS #May1 #M1GS
— AnonymousIRC (@AnonymousIRC) May 1, 2012
Intriguing!
In classic San Francisco fashion, marchers got started last night, some in classic idiot fashion.
Nice work, occupiers. You made me leave my sick kid at home to go clean paint bombs off my windows. That’ll show Wall Street, fellas. #OWS
— Four Barrel Coffee (@fourbarrel) May 1, 2012
So, wherever you go today, don’t be a jerk. We all have different definitions of what constitutes jerkhood. For instance, if you are driving and you find your way blocked by people or bicycles? Don’t mow them down. (At the very least, out of self-interest, because you will go to jail.) If you are demonstrating, please think about what you are shouting or truly demonstrating against. That “the whole world is watching” thing cuts both ways.
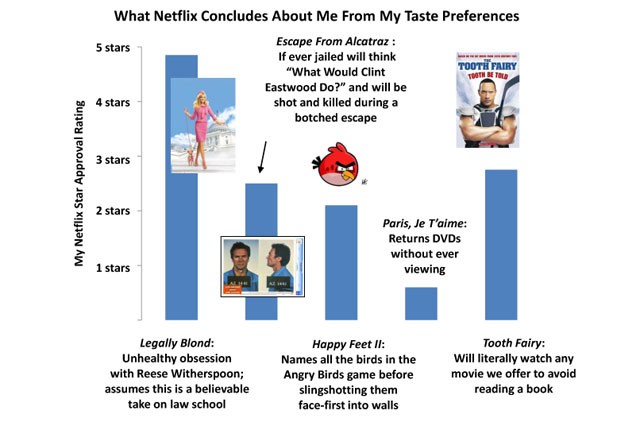
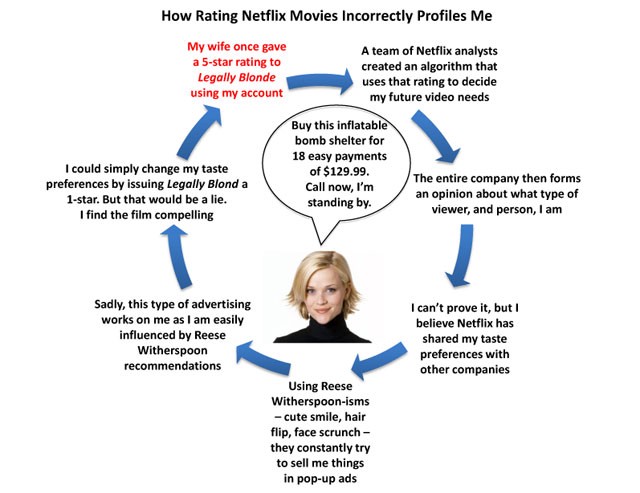
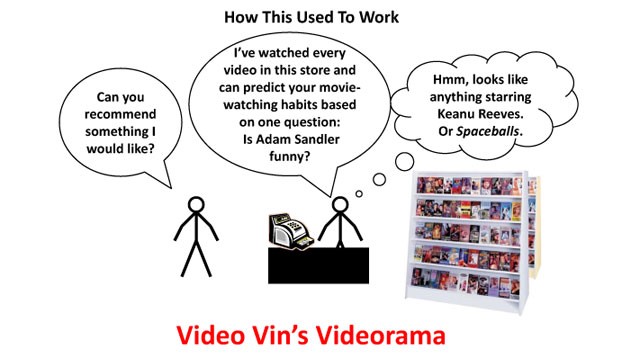
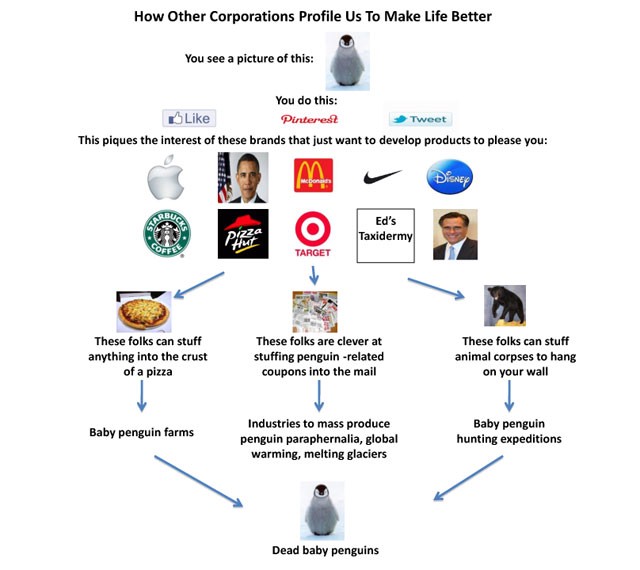
Opinions Netflix Has Formed About Me During My 3.2 Years As Its Customer
Previously: Ways We’ll Pay For These April Temperatures
Jon Methven is the author of This Is Your Captain Speaking, due out in 2012 by Simon & Schuster. He can be reached here, or follow him on Twitter @jonmethven.
Piling on the Hate for LaGuardia
Piling on the Hate for LaGuardia

We have spent a lot of time talking about New York City’s airports (down to our obsession with how to get to JFK from Williamsburg). Our experts’ surprising summation here was that LaGuardia was secretly the most pleasing airport in New York: “You know what the problems are, but it’s quiet in the evenings, has a cool mural and is still the easiest to reach, all other things being equal. Ultimately, the approach up the East River, with Manhattan out the left side window, is one of the most beautiful in the world, every time.” Yeah sure, while that is true, I also particularly like the 50% of LaGuardia landing flight paths with a 45-degree last-minute port-side turn that causes the person behind you to scream. I particularly despise going to LaGuardia, and generally refuse: it’s like waiting for a shuttle at the side of the road in Latvia. So here we are with the Travel and Leisure American airport rankings, sigh, where LaGuardia is ranked the very worst airport in the US of A. Yeah, let’s be honest, it just sucks. And JFK and Newark took fourth- and fifth-worst, but that’s crazy, don’t be talking smack about my JFK. That ranking is only so low because 1. frequency of use creates enmity and 2. Travel and Leisure is read by people who are too wealthy to have done the LIRR to AirTrain magic.
System Kinda Working, Some Days At Least
“Critics have argued that there may still be indirect sources of cow protein in feed (cow protein is fed to chickens, and poultry leftovers go back into cow feed), so more stringent regulations are needed. While those critiques are valid, this case of BSE at least reveals the testing system in the US is not entirely broken.”
— Oh thank God.
Spaaaaaaaaaaaaaaaaaaaaaaaaaace
If you put on your headphones and expand this clip to fill your screen you can imagine that you are deep in outer space, watching the planets, far away from your home and all the problems that plague your life. It’s just you and Saturn and… nothingness. Sweet, sweet nothingness. The calming joy of oblivion. Anyway, it’s a pretty cool video. [Via]
Ear Tells All
“Police in Germany said on Sunday they had solved a series of 96 burglaries by identifying the culprit using the earprints he had left at the scenes while listening at doors.
Killer Mildly Regretful
“Thinking back he wasn’t a bad bloke, actually.”
— “A convicted killer has told a jury how he strangled his neighbour with a TV flex after he flew into a rage following unwanted sexual attention.”
Inside Hermès' Birkin Bag Assembly Line

Did you see this photo series of women making Birkin bags at the Hermès atelier? No reason, just kind of fascinating and porn-ey and like, artisanal sweatshop, in the Olden Times manner. (Happy May Day eve!)
Vancouver's Supervised Drug Injection Center: How Does It Work?
by Paul Hiebert

Vancouver, Canada is the only city in North America that provides a legal facility for drug addicts to push heroin and cocaine and other types of substances into their veins. It’s called InSite, and it’s both government-sanctioned and government-funded.
Located in Vancouver’s notorious Downtown Eastside — often called Canada’s poorest postal code — the supervised injection site opened as a 3-year experiment back in 2003 to curb the neighborhood’s high levels of disease spread through shared needles and death from overdose. Now, after nearly a decade of academic research, political debate, public scrutiny and a Canadian Supreme Court ruling last September that stated InSite should remain open indefinitely, Montreal, Toronto, Ottawa and other cities across the nation are contemplating opening their own injection facilities. According to InSite’s own records, between 2004 and 2010 they had 1418 overdoses without a single one resulting in death. No one has ever died there.
I spoke with Tim Gauthier, InSite’s current clinical coordinator and registered nurse, about the difficulty of maintaining order in a room where most people are high, the significance of whether addicts live or die, and what hope can look like in such an unusual place.
Paul Hiebert: So, how would you describe InSite to someone who’s never heard of it?
Tim Gauthier: It’s place where staff members and nurses supervise people’s injections. The participants come in with their own drugs. In case a participant overdoses or has a heart attack, someone is there to help. If we can intervene timely and quick, there’s no reason anyone should ever die. That’s our primary function.
There was a big push to get a facility like this opened in the late ’90s when overdose rates in British Columbia were reaching epidemic proportions. I think in 1997 we had something like over 450 overdose deaths in the province. Those are absolutely needless deaths.
Participants at InSite have their own booth, which is clean and sanitary. We offer them new needles, alcohol swabs, a sink to wash their hands and medical care. We can dress their wounds and address chronic health issues. We can also link them up with income assistance and housing.
At our front desk, people can pick up equipment such as condoms, lubrication, needles, cookers, filters and everything you need for injecting safely. We give out as much as people think they need. You could take hundreds of needles if you want. There’s no limit. It’s not a one-for-one needle exchange.
Also, we ask that participants maintain the confidentiality of others who use the site.
Most of the people using InSite are not casual, weekend users. Is that correct?
Typically, participants are people who have been addicted for two years or longer. They’re usually heavily addicted middle-aged men from the neighborhood. We also have an overrepresentation of aboriginal users in comparison to general population rates.
We do have the odd time when a person comes in who’s relatively new to their addiction. Maybe they’re not even addicted at all. Either way, they’re new to using. We used to have a blanket rule that we couldn’t accept anybody who was brand new to drugs. But that’s been revamped because we were turning away people who were using one needle several times or injecting alone. They were engaging in much higher-risk behavior.
Why are there so many drug addicts in Vancouver’s Downtown Eastside?
The Downtown Eastside has become a centralized area for poverty. It’s one of the last places in Vancouver that has any level of affordable housing. Vancouver is also a harbor city, so drugs come here easily.
But for anybody injecting their own street drugs, they do that themselves. Nurses can’t poke anyone’s skin with a needle or push the drugs into the participant’s body. However, we can help them find safer veins to reduce the harm they’re doing to their bodies.
InSite is open from 10:00 a.m. to 4:00 a.m. everyday, including holidays. How many people come through InSite per day?
I think before we opened, the experts and scientists and people-in-the-know estimated we’d have maximum 600 visits per day. We’re currently seeing about 800 visits — that includes repeat participants — and sometimes up to 1200. We have thousands of participants registered with us, so we’re well over max capacity of what we anticipated.
Out of those visits, the majority of them are for injections, but people also come to see our alcohol and drug counselors, and to talk about getting into our detox program. Some are there just to access our nursing care. We’re open to the community for medical needs.
What are the main medical ailments you deal with on a regular basis?
We see a lot of wound care. We’re treating abscesses and cellulitis. We’re also doing a lot of testing for sexual transmitted infections, which is kind of new, such as HIV, Chlamydia, gonorrhea and syphilis. All that fun stuff. We can get people on antibiotics right away. We also do immunizations now, such as Hepatitis A or Tetanus vaccines.
But for anybody injecting their own street drugs, they do that themselves. Nurses can’t poke anyone’s skin with a needle or push the drugs into the participant’s body. However, we can help them find safer veins to reduce the harm they’re doing to their bodies.
This sounds like a nearly lawless environment. Are there any rules at InSite?
The rules are very simple: treat each other with respect. Also, you can’t pass drugs or money at InSite. All trafficking has to happen outside. There’s no wheeling or dealing here.

How do you enforce that? These are typically not the most self-controlled individuals.
We bar people, but quite irregularly. If anybody’s caught passing loaded syringes or flaps of heroin or spitballs of cocaine or even money, we restrict his or her access to InSite. And that includes even if a friend passes, like, a lighter. We usually give a warning first cause we can see the lighter, but we can’t see the flap of drugs or whatever else goes along with that. So if people are passing anything and we’ve already warned them, then we bar them for 24 hours. If it’s still an issue after that, then we bar them until they speak to someone on our management team, which can sometimes take a while. It can be weeks or months. But we try to hold off on doing that because it can mean life or death for someone if they overdose outside while barred.
We also bar participants for threats, intimidation or any kind of assault. Compared to working in the hospital though, these incidents are rare. We call the Vancouver Police Department when safety is compromised, and they are very quick to respond.
Barring someone must be a hard decision, since it conflicts with InSite’s mission.
It is. We don’t want to bar someone, but we do our best to make sure trafficking isn’t happening inside and that InSite is a safe place for everyone.
So do drug dealers just linger outside by the front doors then?
Not too often. A lot of people have respect for the site. At times we’ll have somebody hanging outside doing their business, but we try to move them along and they’re usually respectful. We want to promote InSite’s integrity.
What’s the greatest challenge that nurses at InSite face on a day-to-day basis? What’s the hardest part of the job?
Probably just the overwhelming need. We’re seeing a lot of people that are just really, really sick and really, really entrenched in their addiction. Our resources are limited. We have only two nurses on at a time, and some participants are sick beyond the scope of nursing practice. Like, if somebody’s been stabbed five times in the chest. Or if someone comes in with half his arm eaten up by an infection, he might need surgical removal of that dead tissue, and we can’t do that. They need to see a doctor, and getting people to see a doctor is very difficult. If people are entrenched in their addiction, they don’t have the time or capacity to make an appointment or wait a few days. Getting people the appropriate care is the hardest part.
Often we’ll have lineups of four or five people, and sometimes seeing one person can take as quick as two minutes or up to an hour depending on what it is. We can’t see everybody. And these people are hard to treat in the first place cause there’s issues of trust and histories of trauma. It takes a lot for some people to ask for help, so when they do we try to be as responsive and quick as we can.
Is there any one participant’s story that sticks out in your mind?
There was one participant who I definitely had a soft spot for. She was chaotic. She was super disorganized. Over time she was getting sicker — she was losing her spark, her weight, her energy, and her color was looking bad. She was on our radar.
I approached her to see how she was doing, but she didn’t open up to us very much. She didn’t listen to anything her doctor told her. She just wouldn’t take it in.
One day, when she was extremely sick, she brought us a note from her doctor. It had all these things on it. The note said she was septic. She had cavitating lung lesions and abscesses all along her spine. She also had endocarditis, which is an infection in the lining of the heart. Any of these things by themselves are super serious infections — and she had, like, four or five of them.
I had to tell her what this note meant. She was so overwhelmed when I started mentioning the first couple things. She kept asking, “Am I going to die? Am I going to die?” And I had to tell her, if you don’t take care of this, it’s very likely you’re not going to live through these infections.
It still took us days to get her to a hospital because she just didn’t want to go. She was so scared. One of our staff agreed to take her to the hospital and spent the whole night with her in her room, just stroking her hair and being with her. That, to me, was beautiful.
But this participant wouldn’t stay in the hospital because of her addiction. She needed her drugs. So, we were able to connect her with a local community program that administered antibiotics, which she was too sick to be a part of, but they let her in anyway because it was better than the alternative of no care at all. All the doctors were nervous about this. They thought she’d die.
She has since improved significantly.
I know that’s a long sound bite, but it’s one of my most important stories.
What are the main factors that contribute to a person reaching this point? What turns a person into a drug addict?
Addiction is one of those tricky things that nobody really knows what it is. Is it a biological disease? Are some people hardwired for addiction? Or is it something in your past?
Typically, I tend to believe it’s rooted in trauma. I agree with the work of Dr. Gabor Mate and his book In the Realm of Hungry Ghosts, where he goes into what trauma does to our brains and how it affects us and how it alters our response to drugs, such as opiates or cocaine or crystal meth.
So, at InSite we take the approach of trauma-informed care — we just assume people have been traumatized and have heavy backgrounds. And all that means is that we approach people gently. When someone opens up to you about their past, it’s usually pretty dark. There’s significant abuse.
But determinism aside, people do make a number of decisions that increase their chances of getting addicted. What do you say to people who think drug addicts get what they deserve?
Some people talk about overdoses along the lines of population control, but it’s definitely not a humane argument. It’s not even an effective argument in changing anyone’s mind. I don’t hear people saying that drug addicts should just be left to overdose too often. When I do, it’s a head-shaker. But I usually only see it on blogs or through some asshole commentor — something like that. It’s people who feel safe behind their computer. It’s not very common for someone to say that to my face. I don’t even respond to that kind of bullshit.
What’s the most oft-repeated argument you’ve heard for closing down InSite?
That we’re promoting drug use. Which is so far from what we’re doing. If anything, we’re enabling access to services. That’s all we’re doing. People are using drugs anyway, and they have been since before we opened. We’re not encouraging it.
When participants come to us, we’re ready and eager to talk about detox programs and respite and reducing use. InSite participants are 30% more likely to access detox services than those who don’t come here at all.
We’re not trying to push things on people. I mean, we want people to be abstinent, but that’s not our expectation. Our push is to promote safety and harm reduction.
So how do you balance the line between providing a safe haven for drug addicts and trying to get these people to quit? How do you attempt to reform their habits, if at all?
Well, first, we’re trying to reduce harm any way we can without requiring abstinence. We’re not trying to push things on people. I mean, we want people to be abstinent, but that’s not our expectation. Our push is to promote safety and harm reduction.
The approach we take is to promote self-respect. We’re trying to get people to respect themselves regardless of their addictions or whatever’s going on. It’s pretty much unconditional. We’re not going to meet these people with a bunch of shame. We’re not going to lump our expectations and our hopes onto them. Usually they feel shitty enough themselves. They already know that they fucked up. They’re already their own worst enemy.
We’re in this beautiful position where we’re not family and we’re not friends. We have the capacity to accept them again, easily and openly.
Isn’t there also a concern about how much money InSite costs taxpayers?
People often ask why taxpayers should be paying to enable others to get high. It’s really backward. Research supports that InSite is cost-effective in preventing the spread of Hepatitis C and HIV, which are really expensive to treat and maintain. So it’s cost-saving. Every cost-benefit analysis I’ve seen has supported InSite.
Are supervised injection sites a step toward legalizing hard drugs? Are most InSite staff members in favor of this?
I think most staff members are against prohibition. We’d like people to have access to regulated drugs. I mean, a huge problem with drug use is that it’s an illegal market. There’s no regulation on the quality or control of the substances these people are injecting. So people don’t know how strong it is. You could get a flap of heroin that’s maybe double the strength of what you’re used to, and suddenly you’re overdosing.
If you follow examples, like in Portugal and other places that have regulated the drug market, it seems to have positive effects and benefits.
So most of us would be in favor of, say, prescription heroin, which is already happening in Vancouver right now with the SALOME project. It’s a heroin maintenance program, and has been happening for the past six months to a year. It’s a follow-up to the NAOMI study.
After nearly 10 years, what has InSite taught us about drug addiction?
I think our program has been centered on the idea of harm reduction as a health measure, and that’s shown to be valid. It’s much more effective than the war on drugs or the “just say no” policy.
While the U.S. has a history of needle-exchange programs and individuals advocating for harm reduction, they don’t have a facility quite like this. Do you think the U.S. will ever open their own supervised injection site? Why or why not??
I believe that the U.S. might one day have supervised injection sites. The only thing holding communities back from opening their own is conservative ideologies. All of the evidence supports these facilities, in that they save lives, reduce harm to the users, increase public order and help people get off of drugs by increasing their access to services.
However, I’m not sure about U.S. law regarding supervised injection itself, as InSite had to apply for an exemption from Canada’s Controlled Drugs and Substances Act so that nurses, staff and users would not be charged for possession while on the premises. This is where initiatives of this sort require political buy-in.
The U.S. already exceeds Canada, and more specifically, my left-leaning province, British Columbia, in regards to Naloxone distribution programs, so my hope is that a supervised injection site would not be too far of a leap for the U.S. majority to support. It’s a lot to consider on a federal level, but I can see individual states more affected by the harms of drug use being more ready to support an initiative like this.
Is there anything you’d change about InSite if you could?
I think it could be bigger. Again, one of our biggest challenges is wait-times. Not just for nursing care, but to use the injection room, also.
Drug addicts can act like assholes. How do you deal with the frustration they can cause?
Relationally. We don’t tolerate threats or aggressive behavior toward staff or other participants, but we recognize that people’s lives are really hard. We’re sensitive to their plights and challenges. So, we really try to approach them through relationships. We try to sympathize.
Have the drug addicts you work with taught you anything about yourself?
I think they’ve upped my level of authenticity. You can’t really bullshit a bullshitter. You have to be honest. Staff members don’t have much time for pretentiousness. So that transfers to our personal lives, as well.
Has one participant ever given you hope?
Dean Wilson. He’s the guy who took on the Supreme Court of Canada. He was challenging the Charter of Rights and Freedoms as well as the Controlled Drugs and Substances Act.
He was addicted for decades. It was a really chaotic addiction. He’s always been a huge advocate for InSite, and was the chair of the Vancouver Area Network of Drug Users (VANDU). He used the site for years, then he went through our detox program. He went through it a few times. But since the last time, about a year or two ago, he’s been abstinent.
There was also another participant. If we could pick somebody who would never live a life of sobriety, we’d pick her. She was really messy and her injections were quite bloody. She was deeply entrenched in her addiction. She went through a detox program and now has been clean — by the way, I hate the word clean; I hate it — for years. Now she’s published a children’s book called Hope. She’s the best-case scenario. It’s almost like a made-for-TV movie.
Why do you hate the word ‘clean’?
Because it implies that when you’re using you’re dirty. I think that’s disgusting. I don’t think there’s anything dirty or gross about someone just because they’re sick, just because they have an addiction.
Previously: A Q&A; With A ‘Daily News’ Crime Reporter
Paul Hiebert is a writer in New York. Photos courtesy of Vancouver Coastal Health.